Type 1 Diabetes and Ultra Endurance Sport – Why I don’t use an insulin pump.
All material on this website is provided for your information only and may not be construed as medical advice or instruction. No action or inaction should be taken based solely on the contents of this information; instead, readers should consult appropriate health professionals on any matter relating to their health and well-being.
When people learn I have type 1 diabetes, they often ask me, “Why don’t you just get one of those pump thingies?“.

Some insulin Pumps
If you don’t know what an insulin pump is, it is basically a fancy insulin delivery device – pretty much a sophisticated syringe that you can control with a little mini computer. So instead of having to inject insulin using a needle all day, it has a needle and some tubing1.
Even though I choose not to use an insulin pump, they are still pretty popular amongst type 1 diabetics. I do not believe that pumps are for all type 1’s (myself included), but here are the concrete advantages of having an insulin pump:
- You can take micro doses of insulin. For athletes, this actually has a distinct advantage. Insulin sensitivity skyrockets when you’re exercising, and it is very helpful to be able to take less than a single unit (the smallest amount you can “accurately” measure with a standard insulin pen) for a meal.
- You can customize your basal settings to vary throughout the day, and you can suspend your insulin while you’re exercising. Conversely, when you’re doing injections (such as Lantus, Tresiba or Levemir), you really need to plan ahead for your day – trying to estimate how much (and what type) of exercise you will be doing.
Users may also cite other benefits as well, such as not having to inject as often and being able to adjust insulin dosages in public without the “embarrassment” of disturbing others. For sure these are conveniences, but if you’re just drilling down into how to manage type 1 as best as possible, the advantages of the pump really boil down to the two points above. Other than those two reasons, to me, it’s just a fancy, battery powered, mechanically complicated syringe.
Here are the reasons why I do not use a pump:
- Pumps are expensive. A pump costs between $4,500 to $6,500. That does not include the infusion lines, syringes, and batteries (which amount to ~$1,500 per year). Nor does that include the cost of insulin (varies by dosage needs). To put this in perspective: an iPhone costing $500 is about 1/10th the cost of an insulin pump; add in the fact that your life depends on this device, and the thought of breaking your pump is especially disconcerting.
- A type one diabetic can only stay conscious about a day or two at the most if their insulin pump stops working. Therefore, I need to be carrying spare insulin syringes and vials (or pens) in case of failure. In essence, in addition to carrying a pump, infusion sets, syringes and batteries, I’d also have to carry exactly the same kit as I already pack for my regimen of MDI (Multiple Daily Injections). Because my wife and I go on trips that are as long as 3 months, I am already re-using needles hundreds of times to save packing space on our extended tours.2
- If something DOES go wrong with the pump at the wrong time, it can be fatal.345. A person needs insulin in their body all day long. With an insulin pump, it trickles “background” insulin constantly. If I take injections, there is a special “long acting” insulin that lasts 24 hours. If something happens to a pump, within just a few hours, I’d have no insulin left in my body. Conversely, if something happened to my “long acting” insulin, I’d still have 24 hours to find some more insulin. This is an extremely important consideration because we travel to remote locations, far off the grid. Also, there is always the risk of being robbed. A thief may not be discriminate about what they steal, and if my insulin is stolen, the clock begins ticking.
- When it comes to medical devices, insulin pumps have the highest number of reported problems.6. With 17,000 reports of insulin pump problems in 3 years (and 310 of those resulting in death)7, it is a scary statistic once you consider that only 375,000 Americans are using an insulin pump. Your odds of having a problem with the insulin pump are 1 in 22 and your odds of dying 1 in 1209 every 3 years.
- For an active person, having things attached to the outside of your body is quite inconvenient and uncomfortable. My lifestyle involves long bike rides – often in dusty, muddy, hot, humid, wet or freezing places. Many of the places I find myself exploring would be pump killers (or at least hose snaggers). On top of that, some of our bike trips involve significant altitude changes. Once, my wife and I descended 12,000′ in a few hours on a ride in Peru! These ambient pressure changes can have a significant impact on the distribution of insulin from a pump… those changes are even more meaningful when you’re engaged in exercise.

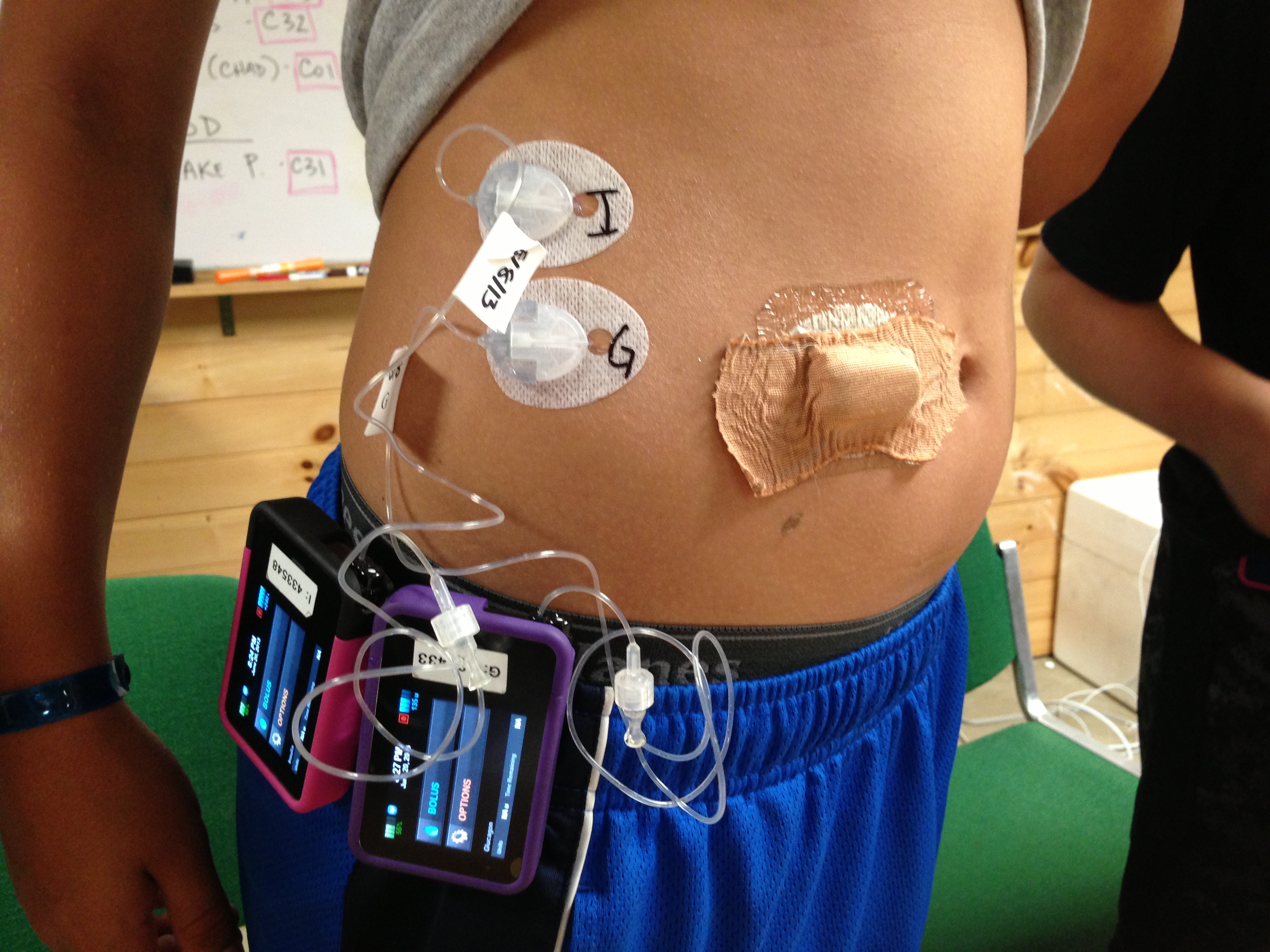
Hmmm… How do you freely jump into a hot spring with this setup attached? This guy is pumping Insulin AND Glucagon, in an attempt to make an artificial pancreas.
- Insulin Availability: Because insulin is necessary for life, whenever I travel, I go to various pharmacies just to ask if they have insulin available. I always carry the insulin I need for a trip from home, but I like to ask for educational purposes.8 In Europe and the US, I’ve found that with a prescription, I can usually get the type of insulin needed for a pump (pumps use “rapid acting insulin”). In Latin America, however, IF a pharmacy has any insulin in stock, it is almost only Lantus, which is used by both type 1 and type 2 diabetics. Type 2 diabetes is common in Latin America, but Type 1 diabetes is rare (and even more rare as you get closer to the equator). While some Type 2 diabetics may use rapid acting insulin, it was not stocked in any of the ~10 pharmacies where I inquired in Mexico and Guatemala. This means that if I were using a pump, I’d have to bring all of my insulin from home (which I already do)… except that I’d need to carry a lot more of the rapid acting insulin, which would take packing space away from my long acting Lantus insulin.
Let’s go back to the positives
Just to be fully objective, let’s look at the other side of the coin. Often times, there are studies that support more than one viewpoint. It turns out that insulin pump users are at a reduced risk of death versus people who take multiple daily injections.9. This data is fairly easy to explain: Because of the cost involved in acquiring an insulin pump, this subset of the diabetic population likely has better access to medicine, diabetes education, and resources than those who cannot afford pumps. The study does indeed cite that “Unmeasured confounders (such as personality, type of care, how often blood sugar is controlled, diabetes education, use of continuous glucose monitoring (CGM), adherence) could affect the results.” Another way to interpret this study is that people with better access to education and medical care fare better than those who do not.
Another positive is that insulin pumps are improving and getting “smarter”. For people who don’t have highly variable activity levels, 10 the newer algorithms for insulin dosing have made things easier for people who use pumps. As technology improves, insulin pumps are becoming more than just “mechanical syringes” as I mentioned at the beginning of the post. Some pumps have algorithms that try and predict your insulin needs and they can distribute the dosages over a period of time that would be challenging to mimic with regular injections. Because of the aforementioned limitations, I still do not believe that any of the currently available insulin pumps are guaranteed to improve the quality of my life. Instead of using a pump, I have pretty good success on my ultra-endurance endeavors using a low carb diet combined with a bolus/basal regime comprised of these four drugs: Lantus/Novolog/Humalog/Afrezza. I have posted about the strategies here.
References & Footnotes
- Note: In the case of the Omnipod, no tubing
- Note: I usually carry about 12 pounds of bikepacking kit (tent, sleeping bag, etc.)… but even with maximal optimization, I still have to carry 2-3 pounds of diabetes gear! Diabetes gear is already a huge fraction of the weight that I carry on extended bike trips.
- Reference: How insulin pumps could give a fatal overdose to diabetics: The ‘foolproof’ alternative to daily injections by LYNNE WALLIS, 2013 http://www.dailymail.co.uk/health/article-2523677/How-insulin-pumps-fatal-overdose-diabetics-The-foolproof-alternative-daily-injections.html
- Reference: MY PUMP ALMOST KILLED ME… TWICE by KATHERINE MARPLE, 2012 https://www.diabeteshealth.com/my-pump-almost-killed-me-twice/
- Reference: FDA Probing Medtronic, Roche And J&J Insulin Pump Injuries & Deaths https://injury-law.freeadvice.com/injury-law/defective_products/defective-insulin-pumps.htm
- Reference: Insulin pumps have most reported problems in FDA database https://medicalxpress.com/news/2018-11-insulin-high-injuries.html
- Reference: FDA Probing Medtronic, Roche And J&J Insulin Pump Injuries & Deaths https://www.freeadvice.com/legal/fda-probing-medtronic-roche-and-jj-insulin-pump-injuries-deaths/
- Note: I always inquire about the cost of insulin when I’m outside of the US. At every pharmacy I’ve been to, a months worth of insulin for me would be about $25-$35 USD. Compare that to over $1,000 in the US!
- Reference: Users of insulin pumps are at 29% lower risk of death compared with patients on insulin injections, 2014, Diabetologia https://www.sciencedaily.com/releases/2014/09/140916182216.htm
- Note: I can have extremely variable activity levels (and thus insulin sensitivities). For example, I may do 10 hours of continuous bike riding one day, and then be sitting in a car for the entire day following. I may be doing a long bike race one day and gardening the next. This highly variable lifestyle means that I’d be constantly having to manage my insulin dosages with or without a pump.

























I wanted to share some (in my opinion) interesting data with regards to the accuracy of blood glucose meters (BGMs). Since my CGM values often turn out unreliable, I do highly rely on my Contour Next One. In the last months, the temperatures have dropped in Switzerland and, especially in the mountains, it can get very cold. I had an intuition that this could affect the readings of my BGM.
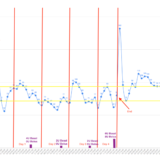
Therefore I devised the following protocol. In my apartment the temperature is rather stable around room temperature (~20C). The temperature outside fluctuates day by day. Over the last couple weeks I have collected data points as follows. First, I would measure the temperature (Tin) and my blood sugar (BGin) in my living room and, then, I would go out, wait for 2 minutes, and measure the temperature (Tout) and my blood sugar (BGout) outside. Then I would record the temperature and measurement difference between outside and inside. I applied simple linear regression to find the following approximate relation: BGout = BGin + 0.0927 * Tin. Note that this formula uses Celsius and mmol/L as units for temperature and blood glucose, respectively.
You can find the data and the fitted curve here (this is the filesharing software of my university): https://polybox.ethz.ch/index.php/s/3T7RlhtdG3966Oj
The interval you find in the graph is the 95% confidence interval and spans from around -0.7 mmol/L to +0.7 mmol/L around the mean. This might seem like a very wide confidence interval, but we have to remember here that I am plotting the difference between two blood glucose measurements. The confidence interval for a single blood glucose measurement would thus be closer to -0.35 mmol/L and +0.35 mmol/L around the mean, which agrees reasonably with my experience of accuracy.
All in all, this data suggests that taking temperature into account when performing blood glucose measurements is very important. If I am up in the mountains, temperatures easily reach 0C or even lower. In this case my measurement will show a value that is 2 mmol/L below the actual value! That is a 33% difference! Extrapolation is dangerous, so I will try to see if I find some way to also collect data for higher temperatures or even lower temperatures.
Hope this was an interesting read.
Greetings from Switzerland
Wouter – Thanks for the information! Like you, I’ve found that the CGM isn’t good for temperature variations (such as the “shower spike” where the CGM reads high, or riding in 0C weather where the readings are off by >50mg/dL). For tight control in a type 1 diabetic, being off by that amount makes the device absolutely useless. It is interesting that you are observing a similar phenomenon with your finger sticks – and it is great that you took the time to collect the data to prove your hunch. My Roche Accu-chek device will not allow me to measure in low temperatures, so when I am camping, I need to keep the meter and strips in my sleeping bag to ensure that the meter will work when it is needed. It sounds like the Contour Next One doesn’t have this software if it is allowing you to test in such low temperatures. Thanks again for sharing this, as I’m sure it will help other people learn more!