Type 1 Diabetes FAQs – You Can’t Eat That, Right?
November is Diabetes Awareness Month, so in the next 30 days or so, I hope to put up some posts for the target audience of non-type-1-diabetics. Confusion about what type 1 diabetes actually means is rampant (even amongst our doctors), and I would like to make my small contribution in clearing up some of the bigger misunderstandings.
- You can’t eat that, right?
- Are you sure you should be eating that?
- Wait, fruit has sugar in it. Are you allowed to eat that?
Some variation of this question comes up every single time I eat something in front of other people who know that I have type 1 diabetes. In fact, I’ll often be sitting in a group, and get the same interrogation more than once in a sitting. When this happens, I try to educate, but whenever I try to explain, the interest in why I’m eating a particular item suddenly evaporates. I have decided to write a post about this sensitive issue and my hope is that I can refer people to the post rather than trying to explain human metabolism at mealtime.
Some type 1 diabetics have resorted to snarky humor to address this common question

The Short Answer
YES! A type 1 diabetic can eat anything that a non-diabetic can eat, provided they have their insulin and blood glucose meter on hand. 1 If my blood sugar is low, you may see me eat fruit or even a baked good. If my sugar is high, I may take an insulin injection and wait until my blood glucose goes down a little before I eat. There is no need to question if I’m allowed to eat whatever I’m eating; I’m constantly making calculations and adjustments in my mind and with my management tools.
The Long Answer
Type 1 diabetes is an extremely complex disorder. I don’t expect anyone without it to come close to understanding how it truly works: When I say, “anyone,” I’m even including our diabetes health care professionals! In order to understand why a type-1 diabetic can actually eat anything that a non-diabetic can eat, we need to understand just a few simple concepts about what type 1 diabetes is:
- A type 1 diabetic’s immune system has destroyed the insulin/amylin producing part of the pancreas.
- With zero insulin, a person will die quickly (less than 24 hours in most cases).
- A working pancreas spends 24 hours a day doing it’s job managing meals, exercise and other assaults to blood glucose stability.
- It is possible for a person to manually take over the 24 hour a day job of the pancreas using the following tools:
- A Glucose Meter
- Injectable Insulin + needles
- A Brain (for calculations/estimations/guess work/compare past results to current conditions/etc.)
- * Not Required, but helpful: Injectable amylin
In other words, if a type 1 diabetic has the first 3 of the 4 listed tools available, they can theoretically eat anything a non-diabetic can! So, where does the confusion come from? Maybe I am responsible for some of the confusion with people thinking I can’t eat certain foods? Maybe people see me delaying my eating or reaching for the low-carb option (which is easier to estimate insulin dosages for)? The reason I generally seek low carb meals is because carbohydrates require more insulin (and also a faster acting insulin) than proteins and fat. So, if I eat a lot of carbohydrate, I need to inject a lot of insulin – and it needs to be of the fastest acting variety. The type and amount of insulin that I inject needs to be as fast and in enough quantity to match the food that I’m eating.

I’ll show you my pancreas if you show me yours! You may have heard the expression “she wears her heart on her sleeve.”… well, I carry my pancreas in my pocket! Here it is, clockwise from top left. 1) Needles 2) Various insulins that last different durations 3) A vacuum bottle to protect my insulin from temperature extremes 4) A phone to keep track of my insulin injections, blood glucose readings, and to help me estimate how much I need to dose. I tend to guess more than rely on the phone, though, because apps are very poor at estimating the effect of exercise. 5) A Spare meter, protected with masking tape (I only bring this on trips, stored in a separate location to protect from theft/loss) 6) My primary meter with a bluetooth Glooko dongle that helps transmit my readings to my phone. **Not pictured: My brain. My brain is monitoring how I feel and making guesses about whether I need to eat or inject most times of the day. That job is normally handled by the pancreas.
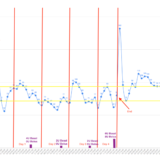
To understand how this can affect me, let’s pretend like having type 1 diabetes is like flying an airplane. In this analogy, if you fly your plane into the ground, you die. If you fly your plane at really high altitude, you get lack of oxygen and exposure to high elevation radiation, which is not good for your long term health. If you don’t have type 1 diabetes, your airplane is on auto pilot 24 hours a day – and you have no idea about the magic your pancreas is conducting behind the scenes. If you DO have type 1 diabetes, you’re in the cockpit of that plane 24 hours a day. This means that when you’re at a dinner party, sleeping, or riding your bike, you need to be constantly aware of your airplane’s elevation. A moment of inattention, and your plane can crash into buildings or trees (I’ll call this hypoglycemia). If you crash all the way to the ground, it is game over – forever.

See the two steering wheel like things? It’s called a “yoke.” If you pull back on the yoke, the airplane goes up. If you push forward, the airplane goes down. In our analogy, eating food is like pulling back on the yoke. Eating fat gently pulls back, eating protein pulls back a little faster, eating carbohydrates pulls back rapidly. Meanwhile, injecting insulin pushes forward, sending the airplane downwards. Exercise can push or pull the yoke dramatically either way, depending on intensity. It’s like turbulence.
If you’ve ever been on a commercial airline, you probably know that the ride is a lot less scary if the plane does not make erratic movements up or down. It is the same way with diabetes. If I inject a lot of fast acting insulin all at once so I can eat a piece of cake, the cake will start yanking back on the yoke to send me to the sky. Meanwhile, the insulin I injected will start shoving the yoke forward to send me back towards the ground. The goal is to have these two forces balance out so that you actually maintain a level flying altitude. No motion sickness, just a sweet awesome day of flying. Sometimes type 1 diabetics nail this type of flying perfectly. It is a cause for celebration and high-fives! Unfortunately, if you don’t get the timing and dose just right, you may be skimming the tree-tops or flying up in the stratosphere, neither of which feel good.
This is where the biggest challenge of diabetes comes in. Non-diabetic can not comprehend this challenge. Many people think that you just inject your insulin and eat some food, and the problem is solved. The issue is: What if the insulin starts working before the food? What if the food starts digesting before the insulin? What if you miscalculated the insulin amount (it changes every day – even hour to hour)? What if your insulin has been out of the refrigerator too long? All of these things can happen in daily life! Insulin absorbs much more quickly if my skin is warm (like if I just took a shower). Insulin absorbs slowly if I’m dehydrated (like after a bike ride). Insulin is MANY times stronger if I just finished exercise – and WAY stronger if I am engaged in exercise. None of these factors are quantifiable – which is why hour-to-hour, dosages and timing are all guesswork. Meanwhile, on the food end, how food is prepared makes a huge difference. A poignant example is a potato. If I eat a potato raw, it does not pull back on that yoke at all.. but if the potato is baked, then it yanks back roughly on the yoke surging my plane towards the sky. What if the potato is cooked “in between?” What if I go to someone’s house for dinner and they say that there is “nothing but oil and vinegar” on the salad… but then I later find out that the vinegar is balsamic vinegar with sugar added. My plane gets rocketed upwards because I didn’t anticipate that I’d have to counteract that with the appropriate amount of insulin.
As you can imagine, this is a lot of turbulence, but it does not mean that I cannot eat certain foods. It does mean that I need to test out certain foods, preparation methods, insulin dosages, and timing in the comfort and safety of my own home. It means that if I’m eating something new, I need to check my altimeter frequently, and make adjustments to the yoke (either through eating sugar or injecting more insulin) over the course of the next 3-4 hours.
But I saw you eat 3 raspberries. I thought you couldn’t eat fruit because it has sugar in it?
In light of what I said above about manually flying this airplane, you can probably see that I need to frequently make adjustments to either point the nose of the plane downwards or upwards. If I’m heading quickly towards the ground, I’m not going to push the yoke forward and accelerate my descent. Instead, I’m going to pull back a little so that I can head upwards a little. The way to pull back on the yoke, and gain a little altitude is to eat something with sugar in it. That is why you may see me sometimes eating a piece of fruit, part of a granola bar, a muffin, or maybe a sugar tablet. I’ll use whatever is on hand (with preference to the sugar tablet) to make a small, gentle altitude adjustment. What I’m saying here is not only CAN I eat something with sugar in it – I actually NEED to eat a little sugar or else when I’m flying low, I risk crashing into the trees.
What I eat, and when I eat it is not based on any type of dogma. I used to pride myself on being the “garbage disposal” where I would eat all the leftovers that people were otherwise going to throw away. Now, with type 1 diabetes, I have to time my eating so that it fits around exercise and insulin injections. Injected insulin is slow to react (and persists for 3-4 hours) which contrasts sharply with the “autopilot” insulin from a normal pancreas (can adjust in seconds). This means that type 1 diabetics need to make plans and calculations for before and after they eat something, but it does NOT mean that any foods are restricted.
Thank you for reading this far, and I really hope that this brings some clarity to this very frequently asked question!
References & Footnotes
- Note: Having Man-made amylin (the other hormone missing in type 1 diabetics) on hand helps make it even easier to eat certain foods.